This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc.
Copyright © 2019Med Learning Group. Built by Divigner. All Rights Reserved.
Ocular diseases, such as diabetic retinopathy (DR), age-related macular degeneration (AMD), and glaucoma affect people of different races, genders, and ethnicities in various ways. Some population groups are more likely to develop certain ocular diseases for physiological reasons. However, access to care and other disparities can also affect the quality of healthcare many people receive, which, in turn, can affect disease prevalence and outcomes.1 Here are several examples of how certain ocular diseases, including retina-related ones, affect people of different races, genders, and ethnicities:
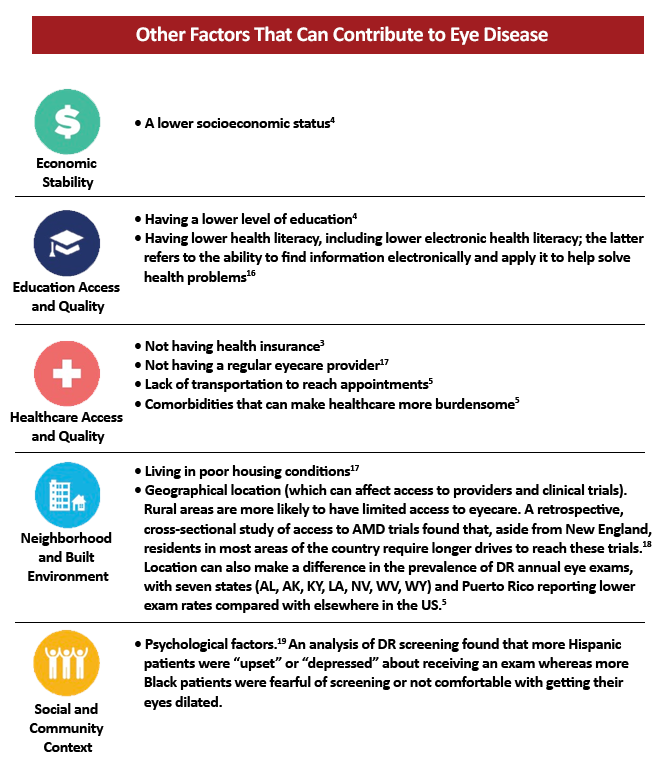
As mentioned previously, other factors beyond physiological reasons can contribute to the prevalence of eye disease in certain population groups. Many of these factors fall under the umbrella of social determinants of health, defined by the US Department of Health and Human Services as “conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.”15
Social determinants of health are grouped under five categories: Economic Stability, Education Access and Quality, Healthcare Access and Quality, Neighborhood and Built Environment, and Social and Community Context. Within eyecare, several prominent social determinants of health can contribute to the prevalence of eye disease including:15
Recognizing a greater need to assist population groups that are more vulnerable to certain ocular diseases, the field of ophthalmology as a whole is making efforts toward improvement. Below is a sampling of some of the changes underway on the organizational, practice, and individual levels:
The American Academy of Ophthalmology (AAO) has its Task Force on Disparities in Visual Health and Eye Care to address health equity in eyecare. This group will help address social determinants of health and medical care, access to care, and outcomes.20
It also has released a collection of seminal articles that address inequities in eye care Telehealth options will likely increase going forward. Telehealth can be a favored option to reach a greater percentage of patients who require care.21 However, physicians and their staff must make sure that patients have access to the technology required for Telehealth and that they are comfortable with it.
Including more patients from underrepresented minority groups in clinical trials can give a broader perspective on side effects and outcomes related to certain treatments.22
Personalized patient education and/or education via video can help increase awareness of health conditions and overcome barriers related to health literacy.16 Sleath et al. conducted a randomized controlled trial focused on encouraging Black patients to ask more questions of their glaucoma providers after watching a video that empowered them to do so. Compared with a control group, the intervention group patients were more likely (odds ratio, 5.4) to ask one or more questions of their providers. This simple type of measure may help improve medication adherence and reduce intraocular pressure23
Reminders regarding health appointments and help with scheduling follow-up are effective ways to ensure that patients maintain eye appointments.24
Adding eye exam lanes to community health centers can highlight the importance of vigilant eyecare24
More eye doctors in “provider deserts” can help reach a broader range of patients who otherwise may not have access to eyecare.24 This approach also gives more patients a stable provider, which can improve adherence to appointments and care.
Identification of patients with lapses in care can be useful both to encourage these patients to seek more frequent eye care but also so providers can make treatment decisions that may last longer compared with patients who can return more frequently.10
Awareness of implicit bias could help address perceptions of disrespect or lack of courtesy perceived by some non-White patients9
Childcare or adult caregiving resources could help patients who do not come for regular appointments due to challenges in these areas9
Artificial intelligence and other new, effective technologies can enhance point-of-care exam for DR among pediatric patients with diabetes. AI-assisted visits led to an exam completion rate of 100% versus 22% among the control group. Of those with an abnormal result, 64% followed up with a provider compared with 22% in the control arm.25
Differences in ocular disease prevalence and outcomes vary widely and encompass a large number of factors. Efforts to make improvements can and should eliminate barriers, ideally improving care for all patients.
This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc.
Copyright © 2019Med Learning Group. Built by Divigner. All Rights Reserved.
